
Sharing my understanding of Ventilation with all of you which is based on self-study, web research, own experience with ventilator and number of cross discussions with device specialists during initial years of this journey. This is just for your reference that how I view these concepts in view of ALS disease behavior. You are free to research more/ add/ correct and form your own logic or follow doctor advice in your situation.
|
|
For beginners: Please refer this video to understand the breathing difficulty stage of ALS patient, which is highly critical to understand and prepare the home with required devices for this transition. If you are able to understand this, you can avoid rushing to hospital in emergency and saved our loved ones from trauma of being in ICU walls.
|
This document is covering following topics
Understand Lungs in view of ALS.
Breathing in and out, is a result of contracting and relaxing the muscles in the chest. And this is partly voluntary (you have noticed that a person can voluntary hold his/her breath) but mainly involuntary. As ALS progresses and motor neuron which control the muscles starts dying, the weakness causes diaphragm to lose strength to help inflate and deflate lungs.
- Understand Lungs in view of ALS.
- Ventilator Terminology
- Understanding ventilator modes
- Devices available for Ventilator@home with their cost and features.
- Few Important points for home ICU setup- including example ventilator settings.
Understand Lungs in view of ALS.
Breathing in and out, is a result of contracting and relaxing the muscles in the chest. And this is partly voluntary (you have noticed that a person can voluntary hold his/her breath) but mainly involuntary. As ALS progresses and motor neuron which control the muscles starts dying, the weakness causes diaphragm to lose strength to help inflate and deflate lungs.
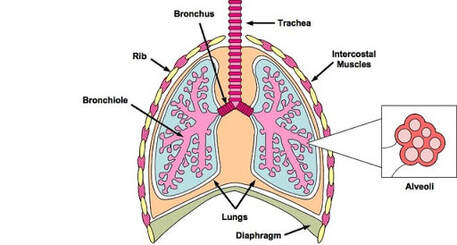
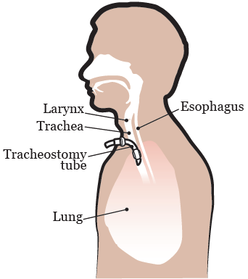
The whole process of breathing intends to inhale more oxygen and exhale carbon dioxide from the body. And this exchange of gases occurs at the level of alveoli of lungs and capillaries of blood via diffusion process. And every time this oxygenated blood transfer cycles to whole body cells. I am referring here mainly about invasive ventilation i.e. tracheostomy -> |
|
Ventilator Terminology
There are major two types of support by Ventilator. Pressure and Volume support. Between this two, Pressure support provided by ventilator breaths mimic human normal staggered flow pattern and more comfortable to patient.
Understanding Ventilator modes
-Both these mode delivers Mandatory breaths only.
-A Mandatory breath is delivered according to the prescribed BPM and inspiratory time settings.
-Ventilator will not respond to patient effort.
Cons – If there is any likeliness that patient wish to breath, machine would NOT let it do, so there is clash (signs- anxiety/uneasiness/uncomfortable). In ALS, breathing capacity gets reduced very gradually, however patient own effort always exists for very long period.
I personally feel this mode should NOT be set at all for ALS patients (and should not be set for 90% other disease patients) , while in reality - usual ICU protocol implements this mode as first mode when person is put on ventilator to everyone (this disturbs the lung state of patient).
-Provides a continuous flow of air at a constant pressure for both inhalation and exhalation to keep the airway open.
-Allow spontaneous breaths only.
Usage – standard of treatment for obstructive sleep apnea, also generally used in the situation when doctors are trying to wean off ventilation.
Cons – It doesn’t ensure that patient get the required number of breaths as all breaths are spontaneous. If patient doesn’t initiate a breath (generally during sleep), number of breaths will reduce→ amount of air exchange reduced→ oxygenation of body reduced.
This is as well standard practice in ICUs to shift to this mode when patient recovers (while ALS case we need BIPAP -and what I came to know that highly advance ventilators in ICUs do not have BIPAP S/T mode)
-This mode provides Spontaneous and Mandatory breaths both.
-A Mandatory breath is delivered if the patient does not spontaneously breathe within the prescribed Breath Rate (BPM) setting. e.g. for a set RR 12, if at
5th second patient didn’t do any effort-ventilator will trigger and complete the breath.
-This ensures that the patient receives a minimum number of breaths per minute (BPM can increase if patients triggers more breaths-so try to see if value can be set <15 initially which gives room for spontaneous breathing).
-In this mode, an IPAP is delivered during inhalation and a lower EPAP (or PEEP) is delivered during exhalation.
-The duration of a Spontaneous breath is determined by the patient effort. The duration of a Mandatory breath is determined by the inspiratory time setting.
AVAPS Average Volume Assured Pressure Support
It is a feature (not mode itself) available which helps patients maintain target tidal volume (VT or Vte). The AVAPS feature adjusts pressure settings by
varying the IPAP level between the minimum (IPAP Min) and maximum (IPAP Max) settings.
Technique behind AVAPS - AVAPS averages tidal volume over many breaths and minutes and this changes to the Pressure settings occurs very gradually,
so it didn’t feel abrupt like in other modes (specially volume)., so that the patient is not aware of breath-to-breath pressure changes.
e.g. If patient is at S/T mode (AVAPS OFF) and Inspiratory pressure is set to 14 for achieving tidal volume 300. Very likely this tidal volume gets delivered
fine initially, however temporarily (may be during situation of unexpected clogging, heavy secretions) or overtime (as gradually patient effort decreases
which leads to receive lower tidal volume e.g. 200.) this cannot compensate the requirement of body oxygenation.
-Mode provides Spontaneous, Assist, and Mandatory breaths.
-This mode uses a time window to decide what type of breaths should be delivered. When you enter PC-SIMV mode, the time window is started. If the
patient does not trigger a breath, the ventilator will provide a Mandatory breath when the time expires and then begin the process again.
This mode may sound like S/T+ AVAPS, however gives less room for patient own breaths as per my understanding. My opinion is to have this mode as
second preference after BIPAP S/T AVAPS.
Devices
- Tidal Volume (generally named as Vt, TV): volume of gas exchanged in each breath cycle. This generally be set referring “body weight in Kg” * 6 to 8. I prefer starting the ventilation with *6 only, as that gives room for increasing the tidal volume in further deterioration in future.
- Peep – (PEEP term used in passive circuit, in active - EPAP) The pressure which remains in the lungs after breathing cycle is complete (inspiration & expiration). This ensure that lungs do not get collapsed
- Minute Ventilation - Amount of air exchange in each minute. (This is equal to = RR*Vt)
- Respiratory Rate/Breath Rate (RR/BR): This is normal respiration rate. (Generally kept between 12-18, most likely 14-15).
- I:E ratio - Inspiratory and Expiratory Ratio. Recommended as 1:2 (e.g. for a 6 second of breath (2:4), inspiratory time set as 2 and it automatically calculates the rest as expiratory time as 4 second).
- Controlled Breath (related to machine breath/mandatory breath): These breaths are completely “controlled” by the ventilator. A ventilator should never be set with controlled breaths only, this is needed only in extreme situation when person in coma/paralyzed or doesn’t have any respiratory drive (under heavy sedation). e.g. Let’s say your ventilator was set up with only controlled breaths at a respiratory rate (RR) of 12 breaths per minute. Every 5 seconds exactly similar breath will be delivered to the person irrespective of anything. If patient has some power and try to take his/her own breath, then there will be clash between the body and the ventilator, which would not allow that breath to happen.
- Spontaneous Breaths: These breaths are triggered (patient’s inhalation effort) by patient himself/herself and depending on other parameters set- ventilator will give person some support (pressure or volume based) to complete the breath.
There are major two types of support by Ventilator. Pressure and Volume support. Between this two, Pressure support provided by ventilator breaths mimic human normal staggered flow pattern and more comfortable to patient.
Understanding Ventilator modes
- CV- Controlled mode or T mode – Timed mode
-Both these mode delivers Mandatory breaths only.
-A Mandatory breath is delivered according to the prescribed BPM and inspiratory time settings.
-Ventilator will not respond to patient effort.
Cons – If there is any likeliness that patient wish to breath, machine would NOT let it do, so there is clash (signs- anxiety/uneasiness/uncomfortable). In ALS, breathing capacity gets reduced very gradually, however patient own effort always exists for very long period.
I personally feel this mode should NOT be set at all for ALS patients (and should not be set for 90% other disease patients) , while in reality - usual ICU protocol implements this mode as first mode when person is put on ventilator to everyone (this disturbs the lung state of patient).
- CPAP -Continuous Positive Airway Pressure
-Provides a continuous flow of air at a constant pressure for both inhalation and exhalation to keep the airway open.
-Allow spontaneous breaths only.
Usage – standard of treatment for obstructive sleep apnea, also generally used in the situation when doctors are trying to wean off ventilation.
Cons – It doesn’t ensure that patient get the required number of breaths as all breaths are spontaneous. If patient doesn’t initiate a breath (generally during sleep), number of breaths will reduce→ amount of air exchange reduced→ oxygenation of body reduced.
This is as well standard practice in ICUs to shift to this mode when patient recovers (while ALS case we need BIPAP -and what I came to know that highly advance ventilators in ICUs do not have BIPAP S/T mode)
- S/T – Spontaneous/Timed
-This mode provides Spontaneous and Mandatory breaths both.
-A Mandatory breath is delivered if the patient does not spontaneously breathe within the prescribed Breath Rate (BPM) setting. e.g. for a set RR 12, if at
5th second patient didn’t do any effort-ventilator will trigger and complete the breath.
-This ensures that the patient receives a minimum number of breaths per minute (BPM can increase if patients triggers more breaths-so try to see if value can be set <15 initially which gives room for spontaneous breathing).
-In this mode, an IPAP is delivered during inhalation and a lower EPAP (or PEEP) is delivered during exhalation.
-The duration of a Spontaneous breath is determined by the patient effort. The duration of a Mandatory breath is determined by the inspiratory time setting.
AVAPS Average Volume Assured Pressure Support
It is a feature (not mode itself) available which helps patients maintain target tidal volume (VT or Vte). The AVAPS feature adjusts pressure settings by
varying the IPAP level between the minimum (IPAP Min) and maximum (IPAP Max) settings.
Technique behind AVAPS - AVAPS averages tidal volume over many breaths and minutes and this changes to the Pressure settings occurs very gradually,
so it didn’t feel abrupt like in other modes (specially volume)., so that the patient is not aware of breath-to-breath pressure changes.
e.g. If patient is at S/T mode (AVAPS OFF) and Inspiratory pressure is set to 14 for achieving tidal volume 300. Very likely this tidal volume gets delivered
fine initially, however temporarily (may be during situation of unexpected clogging, heavy secretions) or overtime (as gradually patient effort decreases
which leads to receive lower tidal volume e.g. 200.) this cannot compensate the requirement of body oxygenation.
- If AVAPS is ON - This allows one to set two inspiratory pressure settings for having a range (min and Max), this automatically increases pressure if temporarily situation comes (clogging or high secretions) and ventilator will come back to normal pressure in absence of any hindrance.
- This helps to maintain the target tidal volume, delay other deterioration conditions and helps many times to overcome emergency.
- Please note- The IPAP level will not rise above IPAP Max, if the target tidal volume is not reached, so over a period we should keep monitoring the ventilator alerts (specially LMV) and take action to shift the range optimum required for that stage. (This range changes shift may be requiring revisiting after year or so)
- PC-SIMV Mode – Synchronized Intermittent Mandatory Ventilation
-Mode provides Spontaneous, Assist, and Mandatory breaths.
-This mode uses a time window to decide what type of breaths should be delivered. When you enter PC-SIMV mode, the time window is started. If the
patient does not trigger a breath, the ventilator will provide a Mandatory breath when the time expires and then begin the process again.
This mode may sound like S/T+ AVAPS, however gives less room for patient own breaths as per my understanding. My opinion is to have this mode as
second preference after BIPAP S/T AVAPS.
Devices
Cough Assist machine E70: (expensive but can be very useful to push tracheostomy stage or any infection reaching to hospitalisation): useful in invasive & non-invasive both

|
CoughAssist E70 is a mechanical insufflation-exsufflation device designed to noninvasively clear secretions from the lungs by simulating a natural cough. Similar to a normal deep breath, CoughAssist gradually applies positive air pressure (insufflation) to obtain a large volume of air within the lungs. The device then quickly reverses the flow of air by shifting to negative air pressure (exsufflation). The resulting high expiratory flow helps mobilize secretions out of the airway as a deep, natural cough would do.
Many of our ALS C & S members are using it to stay away from secretions and thus infection episodes. |
Devices available for Ventilator@home
We used “trilogy 100” continuously 24*7and spent this 8-year journey having this as primary device while “A 40” as backup device (hardly used). So, I am most confident with Trilogy.
Trilogy 100 Price -3.25 -3.80 lacs

|
|
- Power backup -Internal Battery -3 hours + detachable battery 4-5 hours. Also, we used to keep a channelized power supply using UPS for saving it from fluctuations, this background backup with UPS additionally provides 4-5 hours of backup.
- Pressure support range: 4-50 cm H2O
BIPAP A-40 Price -1.6 -2.2 lacs

|
|
BIPAP AVAPS Price -65 -90K

|
|
RESMED 100 Astral 3-3.5 lac

|
|
RESMED 150 steller 2.2-2.8 Lac

|
|
AgVa (2-3 models) 50K-2 lacs

|
|
Few Important points for home ICU setup
Here are few Tips/pointers before you plan for Ventilator or ready with mode and settings required. During my experience dealing in many instances with multiple patients over the years, have seen incorrect use of circuit, mode, tubing, placement of HME, whisper valve, bacteria filter, so trying to list what I consider the best scenario.
Generally, it is assumed that doctors/Ventilator technician who come to install ventilator are expert and we tend to believe them. However, 95% of the times I have observed issues/errors in these settings which has put patient’s life at risk. (You can refer to Shout out page to refer these real experiences)
So, please cross check below points with your setup and if anything, look different- study more in that aspect to reach to conclusion before you try to apply changes.
Example case for Ventilator settings
Now come to couple of important alarms, (for example parameters above, minute ventilation is 360*15=> 5400 or 5.4) so you can be alerted for action required. What I observed, generally it averages out last 3-5 breaths taken and give alarms for the threshold decided.
Low Vte – optional as LMV alarm is there.
High Vte- optional as HMV alarm is there.
LMV (Low Minute Ventilation)- 4
HMV (High Minute Ventilation)- 8
Low Vte and LMV alarms – if this alarm coming temporarily, both will help alert the condition of secretion plug blocking airway passage. One should immediately do trachea suction in this situation. If this alert is regular- either your value of alarm is wrongly set, or pressure range need to be shift to high. (e.g. 12-20 to be changed to 14-22)
High Vte or HMV alarm – generally you will get during coughing, after trachea suction or anxiety
Thumb rule to know the pressure settings are, when patient is calm and awake, please monitor ventilator screen to understand how much pressure is getting utilized (e.g. 14) to achieve the tidal volume. Generally, we can keep Ipap (min) as -2 and Ipap (max) as +4 or +6 of that value (14), so range in this case is 12-20.
BIPAP term is commonly used for device which is used during non-invasive ventilation (whole issue is Philips respironics has patented this term BIPAP and device are named accordingly), While it is actually a method of delivering air to lungs no matter it is invasive or non-invasive. There is general myth that having someone using BIPAP S/T on tracheostomy is considered lower modes while it is ‘the mode’ suitable for ALS patients as they continue to maintain their breathing effort (with very gradual decline over years). Also incorporating AVAPS ensures average of breaths is maintained and that change is so smooth that it doesn’t disturb the patient.
Also refer to following useful, already compiled information 2015:
Some procedure tips :
http://alslifemanagement.weebly.com/learnings.html
Requirement for build Home ICU setup and kind of procedures and their frequencies.
http://alslifemanagement.weebly.com/home-vent-care-management-procedures-equipments-and-required-supplies.html
Ventilator document: Document written by Satvinder Kaur for knowledge sharing with ALS Care and Support group at India.
Qualification : B.Sc. medical, Masters Computer Management.
Working as Database Architect with IBM.
Disclaimer: Please just refer this document for your knowledge and I do not claim it be medically certified information. You are free to research more/add/correct and build your own logic or follow doctor advice in your situation.
Here are few Tips/pointers before you plan for Ventilator or ready with mode and settings required. During my experience dealing in many instances with multiple patients over the years, have seen incorrect use of circuit, mode, tubing, placement of HME, whisper valve, bacteria filter, so trying to list what I consider the best scenario.
Generally, it is assumed that doctors/Ventilator technician who come to install ventilator are expert and we tend to believe them. However, 95% of the times I have observed issues/errors in these settings which has put patient’s life at risk. (You can refer to Shout out page to refer these real experiences)
So, please cross check below points with your setup and if anything, look different- study more in that aspect to reach to conclusion before you try to apply changes.
- Circuit path is.
- Tracheostomy Tube → Catheter Mount→ HME Filter → Whisper Swirl → long hose pipe which takes to Ventilator → Bacteria filter (optional as HME filter do the purpose here) → Ventilator.
- If using humidifier (we used fisher n paykel MR 850) instead of HME filter, circuit be different. Here hose pipe other end will go in outlet of humidifier while there is another small hose pipe which connects ventilator to humidifier. So, Ventilator delivers the air, pass that air through humidifier and delivers warm & moist air to patient (humidification serves purpose of normal nose).
- Cough Assist machine (expensive as it is >2 lacs of rupees but can be very useful to push tracheostomy stage or any infection reaching to hospitalization): useful in invasive & non-invasive both. Highly recommend this device if finances are not much of concern. https://www.philips.co.in/healthcare/product/HC1098159/coughassist-e70-mechanical-insufflator-exsufflator
- Given an option – please use HME filter than humidifier as the latter makes maintenance more difficult for caregivers due to accommodating many procedures in your routine. We used it as Mumma’s breathing pattern was not doing fine due to HME filter resistance in the circuit.
- If using Philips Respironics Trilogy/A-40 /Bipap AVAPS (for others pls refer your ventilator manual) – For single limb, please make sure Passive mode is selected. (Active mode is where you use another tube supplied for expiation)
- Whenever possible, use single limb circuit in home care as it eases the management of tubing and weight of tubes on patient’s tracheostomy/neck and please use whisper swirl valve.
- Key to Ventilator management is doing tracheal suction correctly.
- I strongly believe that passive S/T BIPAP AVAPS mode is perfect for ALS patients, no matter what the doctors says and that is on basis of 8 years experience of Mumma on Ventilator 24*7 and many case studies internationally in ALS forums. Also, with each passing day of managing many patients through a ALS Care and Support group since 2015, where this mode recommendation and settings helping everyone for a long time on Bipap(non-invasive)/Invasive ventilation.
Example case for Ventilator settings
- Weight: 60 KG (or height basis)
- Tidal volume = 60*6=> 360 (We need to give room for future as we are looking at long term ventilator requirement)
- Ipap (min)= 12, Ipap (max) = 18
- BR/RR = 15
- Inspiratory time = 1.3 . (To get ratio of 1:2 for above. As each breath around 4 second (15*4=>60). It can be set at 1.3. Otherwise one can as well calculate 20/RR=> Inspiratory time.)
- Circuit type is – Passive (make sure you have whisper swirl connector for exhalation)
- Mode - S/T BIPAP
- AVAPS - ON (This feature is of Philips Respironics while Resmed machines have iVaps performing same role)
- AVAPS rate -3
- Trigger Type – Autotrak
- EPAP - 6
- Ramp length - OFF
- circuit disconnect – 5 sec
- Apnea alarm – OFF (as for knowing whether current breath was ‘spontaneous breath’, you can see a blinking dot at the left side of pressure bar).
- Low respiratory rate – 10 (irrelevance here but can keep)
- High respiratory rate - 30
Now come to couple of important alarms, (for example parameters above, minute ventilation is 360*15=> 5400 or 5.4) so you can be alerted for action required. What I observed, generally it averages out last 3-5 breaths taken and give alarms for the threshold decided.
Low Vte – optional as LMV alarm is there.
High Vte- optional as HMV alarm is there.
LMV (Low Minute Ventilation)- 4
HMV (High Minute Ventilation)- 8
Low Vte and LMV alarms – if this alarm coming temporarily, both will help alert the condition of secretion plug blocking airway passage. One should immediately do trachea suction in this situation. If this alert is regular- either your value of alarm is wrongly set, or pressure range need to be shift to high. (e.g. 12-20 to be changed to 14-22)
High Vte or HMV alarm – generally you will get during coughing, after trachea suction or anxiety
Thumb rule to know the pressure settings are, when patient is calm and awake, please monitor ventilator screen to understand how much pressure is getting utilized (e.g. 14) to achieve the tidal volume. Generally, we can keep Ipap (min) as -2 and Ipap (max) as +4 or +6 of that value (14), so range in this case is 12-20.
BIPAP term is commonly used for device which is used during non-invasive ventilation (whole issue is Philips respironics has patented this term BIPAP and device are named accordingly), While it is actually a method of delivering air to lungs no matter it is invasive or non-invasive. There is general myth that having someone using BIPAP S/T on tracheostomy is considered lower modes while it is ‘the mode’ suitable for ALS patients as they continue to maintain their breathing effort (with very gradual decline over years). Also incorporating AVAPS ensures average of breaths is maintained and that change is so smooth that it doesn’t disturb the patient.
Also refer to following useful, already compiled information 2015:
Some procedure tips :
http://alslifemanagement.weebly.com/learnings.html
Requirement for build Home ICU setup and kind of procedures and their frequencies.
http://alslifemanagement.weebly.com/home-vent-care-management-procedures-equipments-and-required-supplies.html
Ventilator document: Document written by Satvinder Kaur for knowledge sharing with ALS Care and Support group at India.
Qualification : B.Sc. medical, Masters Computer Management.
Working as Database Architect with IBM.
Disclaimer: Please just refer this document for your knowledge and I do not claim it be medically certified information. You are free to research more/add/correct and build your own logic or follow doctor advice in your situation.
Site Map:
Home page Life Learnings and Procedures Tips Contact us Testimonials/Blessings Video Gallery Image Gallery Analytics
Dressing Home Vent care management (equipments, procedures and regular supplies) Feed preparation and PEG feeding
Ventilator Shout Out!!! ICU -Build safe ICUs, save lives. Open letter to Indian Government on ALS C & S group demands
Home page Life Learnings and Procedures Tips Contact us Testimonials/Blessings Video Gallery Image Gallery Analytics
Dressing Home Vent care management (equipments, procedures and regular supplies) Feed preparation and PEG feeding
Ventilator Shout Out!!! ICU -Build safe ICUs, save lives. Open letter to Indian Government on ALS C & S group demands
Please help spreading 'ALS awareness' in India.
